A recent paper from the World Economic Forum – the group that runs the Davos conference – stated that Americans pay more for healthcare than other countries but get inferior outcomes. That rhetoric was amplified by Warren Buffett, when he called health care costs a “hungry tapeworm” eating into the American economy. But, before you assume that Americans are not getting good value for their health care dollars, let’s look at the data.
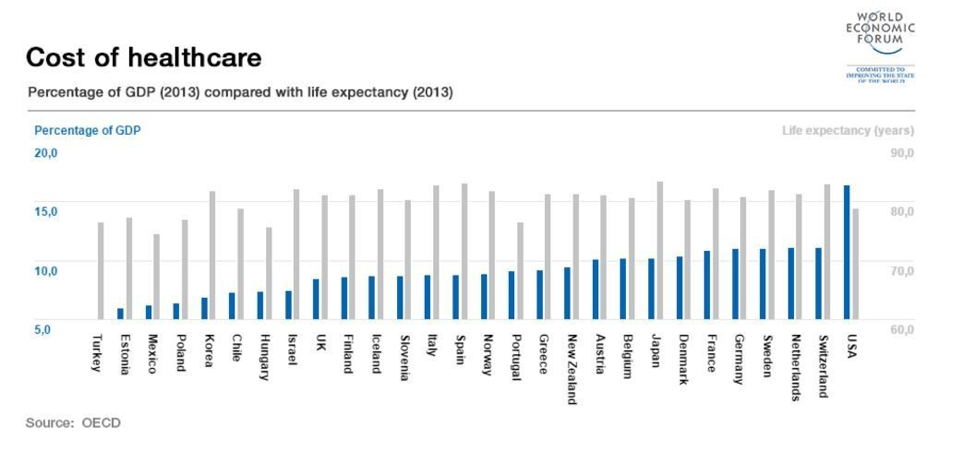
The data (from the Davos paper) at the heart of those claims will be familiar to anyone who has followed health care issues:

The dark blue bars show that the U.S. spends more on healthcare as a percentage of GDP (17.1%) than other developed countries, and the light gray bars show Americans have a lower life expectancy at birth (age 79).
Those facts are not in dispute. The problems are that life expectancy at birth is a highly imperfect measure of health care outcomes and that health care spending as a percentage of GDP doesn’t accurately measure how much a government’s outlays affect the health of its citizens.
The problems with life expectancy at birth
No single metric can accurately measure something as multifaceted as the efficacy of health care spending. But life expectancy at birth is a natural choice for those looking for a simple answer to a complex question. Unfortunately, its simplicity masks its many shortcomings.
Let’s start with the fact that life expectancy at birth is very different for blacks and whites. Data from the Center for Disease Control (CDC) shows that white men can expect to live to age 78.8, black men to age 74.5 and non-Hispanic black men to age 74.2. The pattern is the same for women. Among the reasons blacks have shorter life expectancy is that they are more likely to die from heart disease, cancer, homicide and diabetes. This data raises the issue that the problem with lower U.S. life expectancy is rooted in discrimination and inequality rather than the efficacy of our healthcare.
Incidentally, the same racial pattern exists in infant-mortality rates. The overall rate for the U.S. is 6.1 deaths per 1,000 live births, which is the highest among developed nations. But for blacks the rate is 11.7 and for whites it is 4.8. (The U.S. rates are also elevated in part because it has a higher rate of births before 24 weeks of gestation, which are riskier births.)
Supporting the inequality argument is research that has looked at the differences in longevity based on level of education. Education is a reliable indicator of socioeconomic status and has the advantage of appearing on death certificates. For all subgroups (white, black and Hispanic; male and female), higher education correlates with greater longevity. The largest gain is for white males; those with 16 or more years of education lived 12.9 years longer than those with 12 or fewer years. The smallest gain is for Hispanic females, who lived 2.9 years longer based on the same difference in education.
Higher education translates to greater income and better access to healthcare. This suggests that the issue is not that the U.S. has poor healthcare or health care outcomes, but that it doesn’t provide sufficient access to the poor and poorly educated.
The last problem with using life expectancy at birth as a metric is that homicide rates are very high in the U.S. That, coupled with the opioid epidemic, claims victims who are mostly under the age of 50. Gun-related deaths in the U.S. are approximately 3 per 100,000, which is higher than European and Asian countries (but not higher than Mexico, most countries in South America, Russia and some other eastern European countries).
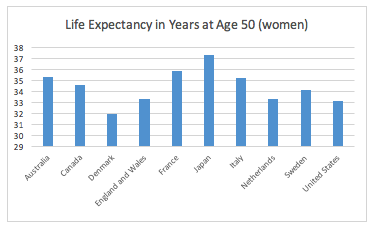
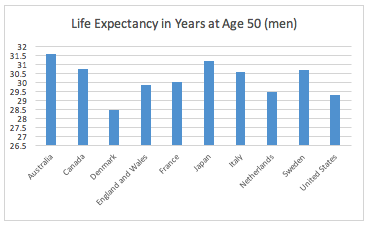
Based on life expectancy at age 50, the U.S. is not the outlier it is at birth (source):
However, recent trends in this data are not encouraging. The gap between the U.S. and other countries has been widening and researchers are unsure of the causes.
There are problems with using life expectancy at age 50 as a measure of health care outcomes. A proper measurement of health care outcomes should be independent of the life style choices of its citizens. However, Americans have made bad choices in at least two areas. The U.S. had the highest per-capita smoking rate for the 40-year period ending in the mid-1980s. A higher portion of the age-50-plus population in the U.S. suffers from the consequences of smoking than in other countries.
Research has shown that if the incidence of smoking in the U.S. was in line with other developed countries, the life expectancies of men and women at age 50 would improve sharply.
The U.S. has a higher rate of occurrence of obesity than in other developed countries, although this is true for those younger and older than age 50. Obesity is closely linked to a number of diseases that shorten lifespans.
A better way to measure health care outcomes
Now that we’ve identified some of the problems with using life expectancy – especially at birth – as a gauge of health care outcomes, let’s look at a better way to measure this.
One way is to measure how successfully a disease is treated, which is a direct function of the health care system and largely independent of life style choices. This measurement is possible with cancer, since disease registries for it exist worldwide. An unbiased way to measure this is the mortality rate (i.e., the five-year survival rate following diagnosis).
By focusing on the survival rate, researchers can measure the efficacy of the treatment. This provides an objective and unbiased way to compare healthcare across counties.
This assumes that patients want to live longer and are willing to tolerate often toxic and painful treatments. It may be the case that non-U.S. health care systems succeed with palliative and hospice care, but this would require a different measurement metric.
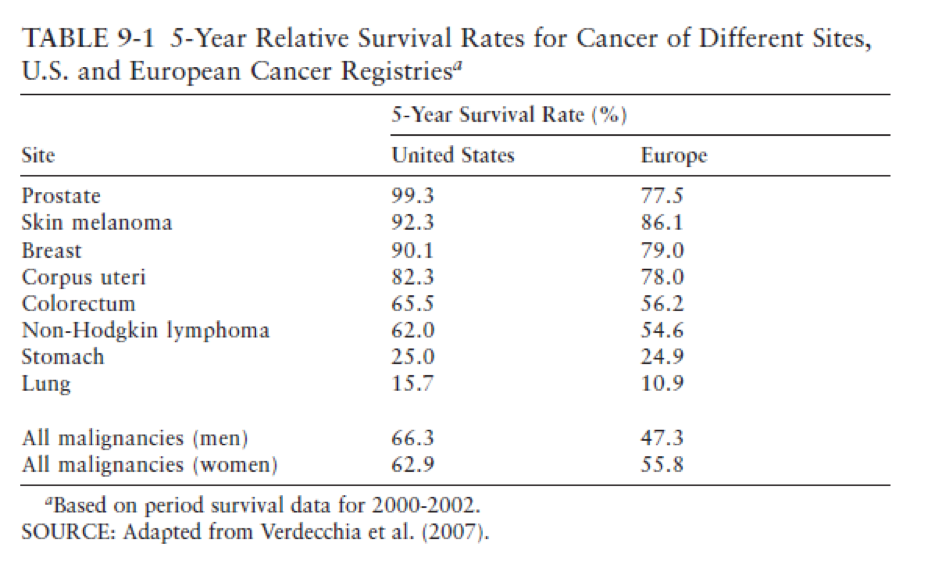
Below are the results for certain types of cancers (source, chapter 9), comparing the U.S. to 17 countries in Europe:
The results for the U.S. are impressive. Indeed, not only did the U.S. outperform the 17-country averages for all types of cancers, it outperformed all 17 countries individually for lung, breast, prostate, colon and rectal cancers.
Another area of research comparing the U.S. to other countries has been for cardiovascular diseases and strokes. But there aren’t national registries for this data, so the findings are much weaker than for cancer. Researchers have found that high blood pressure and high cholesterol are more likely to be treated in the U.S. than other countries. Survival rates after heart attacks are above average in the U.S. but about average after a stroke.
The superiority of the U.S. health care system is evident in the cancer survival rates. If, as one would expect, this superiority extends to other complex or hard-to-diagnose diseases, then one should be very skeptical of claims that the American health care system is not the best in the world.
Health care expenditures as a percentage of GDP
Let’s turn to a separate question. The U.S. spends more, as a percentage of GDP and on a per capita basis, on healthcare than other developed countries.
But that doesn’t tell the full story.
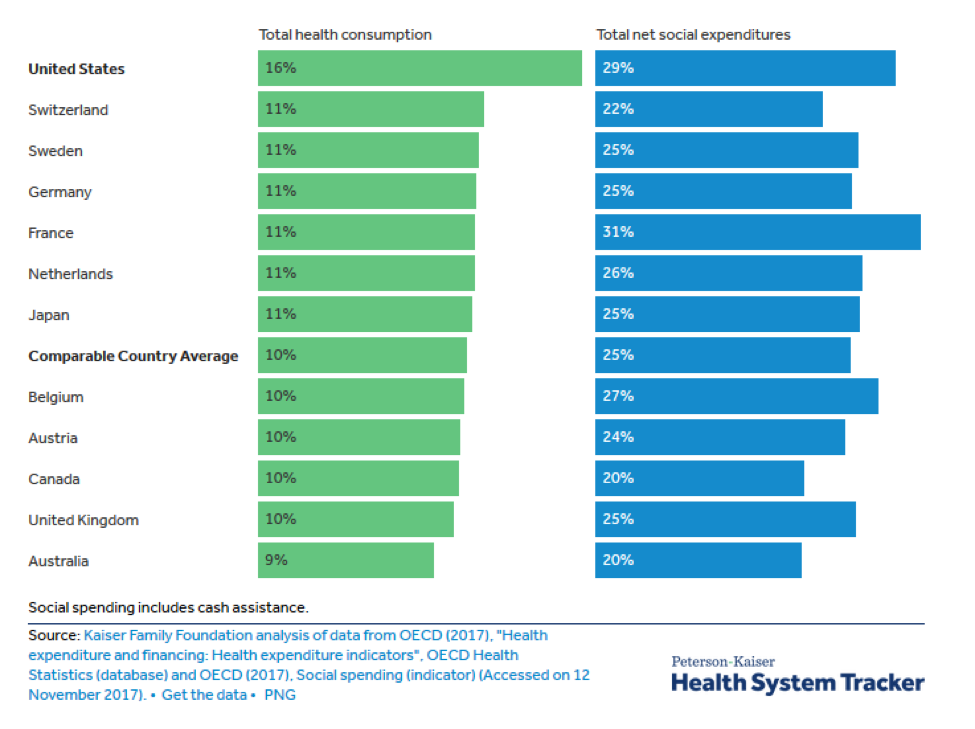
The U.S. spends considerably less than other countries on social services (cash assistance and other support for the elderly, poor, unemployed, and other disadvantaged or vulnerable populations). Those funds support housing, food, clothing and other needs that have a direct effect on health outcomes. For every dollar spent on health services, the U.S. spends $0.56 on social services, but the OECD countries spend $1.70 (see here).
When social-service spending is included with healthcare spending, the U.S. is no longer an extreme outlier among developed countries (source):
The above is true despite the fact that the U.S. has a younger average age (38 versus 42) and smaller percent of the population over the age of 65 (14% versus 18%) than the other countries in this sample.
If we go back to our original question – does the U.S. spend more on healthcare than other developed countries – and instead ask whether the U.S. spends more on healthcare and related social services, then the answer is U.S. spends slightly more than average.
What we’ve learned
Measuring health care-related spending and outcomes is a daunting and complex task. It is foolhardy to look for a simple answer, whether it is in life expectancy or spending as a percent of GDP.
But it is dishonest to condemn the U.S. because it spends more on healthcare as a percentage of GDP or it has shorter life expectancies at birth.
The U.S. has a problem delivering good health care to all its citizens. Blacks, the poor and the poorly educated do not have as good outcomes as whites. We have a problem with homicide, opioids, smoking and obesity.
An unbiased way to measure health care outcomes is with the survival rate of certain kinds of cancers, and, on this basis, the U.S. has an outstandingly good record.
The U.S. spends a lot delivering this health care, but that money does not benefit all segments of its population equally. The rich get better healthcare and pay a high price for it.
It is shortsighted to look only at health care spending when asking whether government outlays provide good health outcomes. One should also look at how much a government spends on health-related services (including social services), not just on healthcare, and on this basis the U.S. is not an outlier.
If you are worried about treating a complex and life-threatening disease – and not the hungry tapeworm that Buffett fears – then you’re best bet is the U.S. health care system.
Read more articles by Robert Huebscher